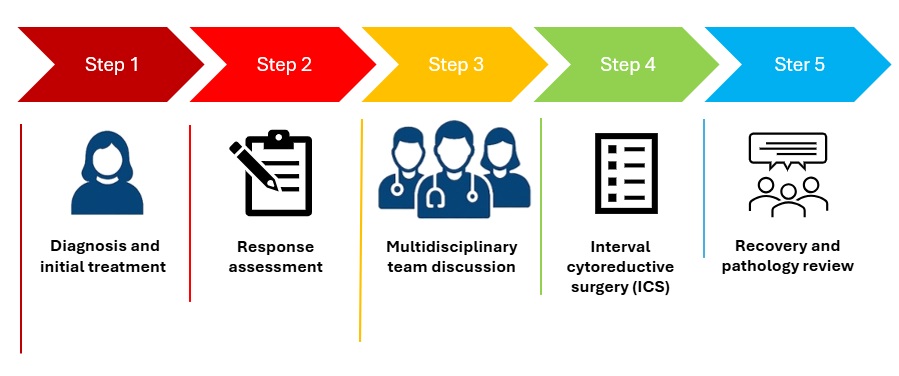
Your treatment pathway
Step 1 – Diagnosis and initial treatment
You are diagnosed with advanced ovarian cancer and start treatment with chemotherapy. This is often the safest and most effective first step.
Step 2 – Response assessment
After a number of chemotherapy cycles, we assess how the cancer has responded. This usually involves scans, blood tests, and review by the multidisciplinary team.
Step 3 – Multidisciplinary team discussion
Your case is discussed by a specialist team including surgeons, oncologists, radiologists, pathologists, and specialist nurses. The team considers whether surgery is safe and whether it is likely to achieve removal of all visible cancer.
Step 4 – Interval cytoreductive surgery (ICS)
If surgery is recommended and you choose to proceed, ICS is planned. This may be after the second or third cycle of chemotherapy, or later (for example after the fourth, fifth, or sixth cycle), depending on individual circumstances.
Step 5 – Recovery and pathology review
You recover from surgery in hospital, supported by the ward, physiotherapy, dietetics, and nursing teams. Tissue removed during surgery is examined by pathologists and reviewed again by the multidisciplinary team.
Next steps
You are seen in clinic to discuss results, recovery, and whether further chemotherapy or other treatment is recommended.
Frequently asked questions about interval cytoreductive surgery
Why not have surgery straight away?
For some patients, starting with chemotherapy is recomended so as to reduce the amount of cancer and make surgery more achievable, with a higher chance of removing all visible disease.
How do you decide when to do ICS?
There is no fixed rule. The timing depends on how the cancer responds to chemotherapy, what scans show, whether surgery is technically achievable, and how well you are physically. Surgery may be considered after three cycles, or later if that gives the best balance of benefit and safety.
What does “complete tumour removal” mean?
This means that no visible cancer remains at the end of surgery. This is strongly associated with better long-term outcomes and is the main goal of ICS when it is safe to aim for this.
Is ICS always successful?
Not always. Occasionally, despite careful planning, it is not safe to remove all disease once surgery has started. In rare cases, surgery may be stopped without proceeding. If this happens, alternative treatment options will be discussed with you.
Will I definitely need a stoma?
No. A stoma is only needed if part of the bowel has to be removed and it is not safe to join the bowel back together straight away. If a stoma is required, this will be discussed with you beforehand wherever possible, and specialist stoma nurses will support you.
How long does recovery take?
Most patients stay in hospital for around 7 to 14 days. Full recovery takes longer and varies between individuals. Fatigue is common, and recovery continues over weeks to months.
Will I need more chemotherapy after surgery?
Many patients do go on to have further chemotherapy after ICS, but this depends on surgical findings, pathology results, and your recovery. This will be discussed with you once results are available.
What happens if I decide not to have surgery?
That is entirely your choice. You will continue to be supported, and other treatment options such as further chemotherapy will be discussed with you.
Who can I talk to if I am unsure?
Your consultant and Clinical Nurse Specialist are key contacts. You are encouraged to ask questions, take time to think things through, and involve family or friends if helpful.
Further trusted information and support is available from ovarian cancer charities such as Ovacome (link to other website).